Frontal lobe syndrome: Difference between revisions


(Original text was in wikiskripta: Syndrom frontálního laloku https://www.wikiskripta.eu/index.php?curid=30258) |
(Translation from czech to english) |
||
| Line 1: | Line 1: | ||
== | ==Anatomical-functional organization of the frontal lobe <ref name="Nevšímalová">{{Cite|type=book|publisher=Galen|edition=1|range=0|year=0000|surname3=Tichý|surname2=Růžička|surname1=Nevšímalová|location=Prague|name3=Jiří|name2=Evžen|name1=Soňa|isbn=80-7262-160-2|title=Neurologie}}</ref>== | ||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
| | |||
}}</ref>== | |||
The cortex of the frontal lobes represents 2/3 of the entire [[cerebral cortex]]. It is separated from the parietal lobe by the sulcus centralis (Rolandi). | |||
=== | === Primary motor area === | ||
It lies in front of the sulcus in the gyrus praecentralis ( area 4, functionally MI). The domstotopic projection corresponds to Penfield's homunculus. | |||
=== | === Premotor area === | ||
It lies on the outer surface of the lobe (area 6). It is superior to the primary motor zone. It belongs to the association zones for movement, it is related to the memory circuits for momentum. By stimulating this zone, we get a much more complex motor response than by stimulating the primary motor zone. | |||
=== | === Supplementary motor area === | ||
It lies on the inner surface of the upper part of the frontal lobe (area 6, functionally M II). The area is connected bilaterally with the premotor area. It ensures posture and body posture, participates in the initiation and planning of [[Free motor skills|free movement]]. The supplementary motor area is involved in cortico-striato-palido-thalamo-cortical circuits. | |||
=== | === Frontal field of view === | ||
It lies in the gyrus frontalis medius (area 8). The corticonuclear pathway to the contralateral visual center in the paramedian [[reticular formation]] of the pontine and in the [[midbrain]]. This area is also sometimes called ''the adverse frontal field'' . If this field is irritated, the bulbs and head will deviate contralaterally. In the case of a lesion of this landscape, the reverse is the case (deviation homolaterally) simultaneously with [[Paresthesia|paresis]] of free gaze contralaterally. The area is part of the reflex arc of optokinetic [[nystagmus]]. | |||
=== | === Prefrontal === | ||
It is quite extensive, it is made up of Brodmann's areae 9, 10, 11, 12. When stimulated, a motor response cannot be evoked, therefore this area is sometimes called the "silent zone". Functionally, it is an association cortical area. | |||
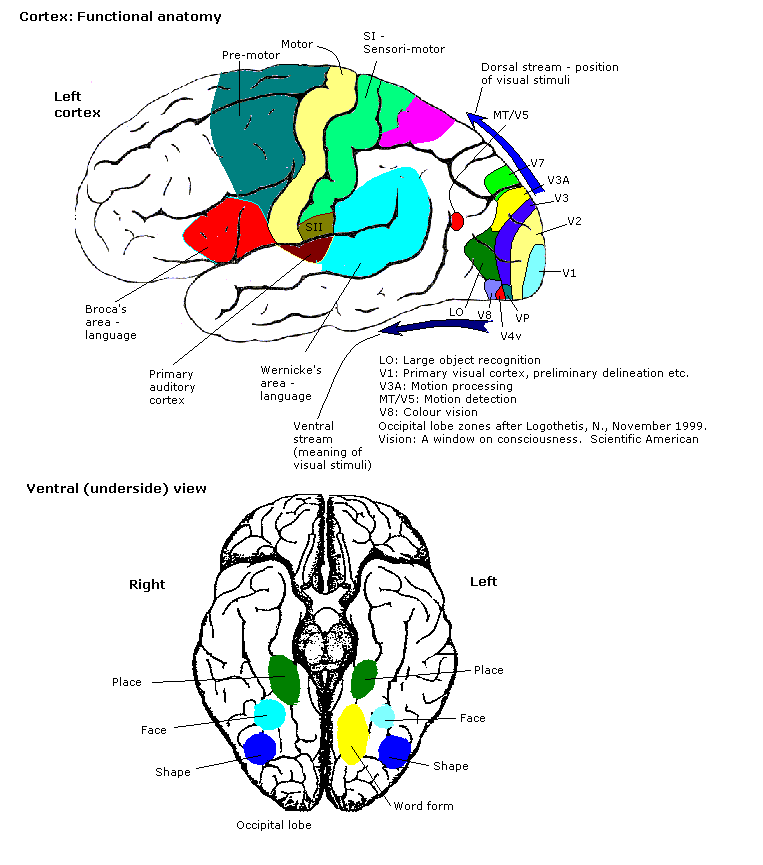
[ | [https://upload.wikimedia.org/wikipedia/commons/d/db/Constudproc.png 280px|thumb|Funkční uspořádání cortexu] | ||
== | ==Frontal lobe dysfunction<ref name="Nevšímalová"/>== | ||
* | * It is associated with movement and [[Behaviour disorder|behaviour]] disorder. | ||
* | * A lesion in area 4 results in '''contralateral central [[paresis]] (plegia)'''. | ||
* | * Bilateral paramedian involvement of area 4 causes '''paraparesis of the lower extremities.''' | ||
* | * Bilateral involvement of the supplementary motor area can lead to '''akinetic mutism and lack of vertical eye movements''' | ||
* | * A lesion in the premotor area results in motor '''[[apraxia]]'''. | ||
* | * When the frontal lobe is affected, we can also encounter '''walking apraxia''', '''[[astasia]]''' (standing with a wide base). | ||
* | * There are '''[[deliberative phenomena]]''' such as the grasping reflex (Janišev), axial reflexes([[Sucking reflex|sucking]], [[Labial Reflex|labial]]), sometimes the feeding reflex (Oppenheim's, "eating"). | ||
* | * The patient '''loses sphincter control''' , sometimes '''gatism''' (smearing of stool) | ||
* | * Affective '''disorders , loss of inhibitions and social feeling''' '''[[bulimia]]''', '''aggressiveness , apathy , abulia''' are common . | ||
=== | === Division of disorders according to the cortical area involved in the corresponding [[Basal ganglia|basal ganglia circuit]] === | ||
* ''' | * '''Dorsolateral prefrontal syndrome''' – affected executive [[cognitive function]] (targeted action, problem solving, learning, [[memory]]). | ||
* ''' | * '''Orbitofrontal syndrome''' – corresponds to the classic [[prefrontální syndrom|prefrontal syndrome]] with disinhibited behavior and emotional lability accompanied by euphoria, puerilism and moria. | ||
* ''' | * '''Anterior cingulate (mediofrontal) syndrome''' – accompanied by depression, apathy and akinetic mutism. | ||
=== | === Other syndrome === | ||
''' | '''Frontal neglect syndrome ([[neglect syndrome]])''' | ||
It is relatively rare. It occurs when the front part (white matter) of the frontal lobe is affected. Simulates bilateral limb paresis.. [[Reflexes]], [[sensation]] (including response to nociceptive stimulus) and electrophysiological parameters are, however, unchanged. The patient may neglect half of the visual field, even if the visual field is intact. Similarly, he may consider his hand to be alien (alien hand, usually left). [[Pyramidal phenomenon|Janišovsky's grip]] tends to be positive. The syndrome must be distinguished from [[anosognosia]] of [[hemiparesis]] or anosognosia of blindness in the case of a lesion of the thalamoparietal speech non-dominant hemisphere (bound to the parietal lobe). | |||
''' | '''Foster Kennedy syndrome''' occurs in tumors of the base of the frontal lobes when the tumor presses on the [[optic fasciculus]] . [[Congestive papilla]] , [[intracranial hypertension]] , unilateral [[hyposmia]] and psychological changes follow | ||
With a lesion of the base of the frontal lobe, there is hyposmia to anosmia. | |||
== | == Causes of damage to the frontal lobes == | ||
* [[ | * [[Brain tumors|Tumors]] | ||
* [[ | * [[Stroke|Strokes]] | ||
* [[ | * [[Inflammation]] | ||
* [[ | * [[Trauma|Traumas]] | ||
<noinclude> | <noinclude> | ||
== | == Links == | ||
=== | === Related articles === | ||
* [[ | * [[Prefrontal syndrome]] | ||
* [[ | * [[Rolandic syndrome]] | ||
* [[ | * [[Occipital lobe syndrome]] | ||
* [[ | * [[Parietal lobe syndrome]] | ||
* [[ | * [[Temporal lobe syndrome]] | ||
* [[ | * [[Functional cortical areas]] | ||
=== Reference === | === Reference === | ||
Revision as of 13:27, 18 December 2022
Anatomical-functional organization of the frontal lobe [1]
The cortex of the frontal lobes represents 2/3 of the entire cerebral cortex. It is separated from the parietal lobe by the sulcus centralis (Rolandi).
Primary motor area
It lies in front of the sulcus in the gyrus praecentralis ( area 4, functionally MI). The domstotopic projection corresponds to Penfield's homunculus.
Premotor area
It lies on the outer surface of the lobe (area 6). It is superior to the primary motor zone. It belongs to the association zones for movement, it is related to the memory circuits for momentum. By stimulating this zone, we get a much more complex motor response than by stimulating the primary motor zone.
Supplementary motor area
It lies on the inner surface of the upper part of the frontal lobe (area 6, functionally M II). The area is connected bilaterally with the premotor area. It ensures posture and body posture, participates in the initiation and planning of free movement. The supplementary motor area is involved in cortico-striato-palido-thalamo-cortical circuits.
Frontal field of view
It lies in the gyrus frontalis medius (area 8). The corticonuclear pathway to the contralateral visual center in the paramedian reticular formation of the pontine and in the midbrain. This area is also sometimes called the adverse frontal field . If this field is irritated, the bulbs and head will deviate contralaterally. In the case of a lesion of this landscape, the reverse is the case (deviation homolaterally) simultaneously with paresis of free gaze contralaterally. The area is part of the reflex arc of optokinetic nystagmus.
Prefrontal
It is quite extensive, it is made up of Brodmann's areae 9, 10, 11, 12. When stimulated, a motor response cannot be evoked, therefore this area is sometimes called the "silent zone". Functionally, it is an association cortical area.
280px|thumb|Funkční uspořádání cortexu
Frontal lobe dysfunction[1]
- It is associated with movement and behaviour disorder.
- A lesion in area 4 results in contralateral central paresis (plegia).
- Bilateral paramedian involvement of area 4 causes paraparesis of the lower extremities.
- Bilateral involvement of the supplementary motor area can lead to akinetic mutism and lack of vertical eye movements
- A lesion in the premotor area results in motor apraxia.
- When the frontal lobe is affected, we can also encounter walking apraxia, astasia (standing with a wide base).
- There are deliberative phenomena such as the grasping reflex (Janišev), axial reflexes(sucking, labial), sometimes the feeding reflex (Oppenheim's, "eating").
- The patient loses sphincter control , sometimes gatism (smearing of stool)
- Affective disorders , loss of inhibitions and social feeling bulimia, aggressiveness , apathy , abulia are common .
Division of disorders according to the cortical area involved in the corresponding basal ganglia circuit
- Dorsolateral prefrontal syndrome – affected executive cognitive function (targeted action, problem solving, learning, memory).
- Orbitofrontal syndrome – corresponds to the classic prefrontal syndrome with disinhibited behavior and emotional lability accompanied by euphoria, puerilism and moria.
- Anterior cingulate (mediofrontal) syndrome – accompanied by depression, apathy and akinetic mutism.
Other syndrome
Frontal neglect syndrome (neglect syndrome)
It is relatively rare. It occurs when the front part (white matter) of the frontal lobe is affected. Simulates bilateral limb paresis.. Reflexes, sensation (including response to nociceptive stimulus) and electrophysiological parameters are, however, unchanged. The patient may neglect half of the visual field, even if the visual field is intact. Similarly, he may consider his hand to be alien (alien hand, usually left). Janišovsky's grip tends to be positive. The syndrome must be distinguished from anosognosia of hemiparesis or anosognosia of blindness in the case of a lesion of the thalamoparietal speech non-dominant hemisphere (bound to the parietal lobe).
Foster Kennedy syndrome occurs in tumors of the base of the frontal lobes when the tumor presses on the optic fasciculus . Congestive papilla , intracranial hypertension , unilateral hyposmia and psychological changes follow
With a lesion of the base of the frontal lobe, there is hyposmia to anosmia.
Causes of damage to the frontal lobes
Links
Related articles
- Prefrontal syndrome
- Rolandic syndrome
- Occipital lobe syndrome
- Parietal lobe syndrome
- Temporal lobe syndrome
- Functional cortical areas
Reference
- ↑ Jump up to: a b NEVŠÍMALOVÁ, Soňa – RŮŽIČKA, Evžen – TICHÝ, Jiří. Neurologie. 1. edition. Prague : Galen, 0000. 0 pp. ISBN 80-7262-160-2.

{kind=link}