Steatosis


Steatosis is an abnormal accumulation of lipids in the cells of parenchymal organs. It is caused by a metabolic disorder with intracellular accumulation of an abnormal amount of lipids.
Manifestations of steatosis[edit | edit source]
Microscopically, we can see fat droplets in the cell free in the cytoplasm or surrounded by a membrane. Many droplets may be present (small-droplet steatosis) or one large droplet (large-droplet steatosis), which suppresses the organelles of the cell at the periphery.
Macroscopically, the organs are yellow (bloody to orange), greasy on section. The cells of parenchymal organs – liver, kidneys, heart and skeletal muscles – are most often affected. The causes of steatosis are mainly obesity, alcohol, diabetes mellitus, but also toxins, hypoxia and protein-calorie malnutrition.
Division of steatosis according to the mechanism of formation[edit | edit source]
Steatosis can arise from a malfunction of some cell organelles – endoplasmic reticulum, mitochondria or lysosomes.
Disorder of synthesis and secretion of lipoproteins[edit | edit source]
A disorder of the endoplasmic reticulum that is unable to produce apoprotein B or MTP (triacylglycerol transfer protein). It therefore affects the cells that create lipoproteins - hepatocytes (VLDL, Apo-B-100) and enterocytes (chylomicrons, Apo-B-48). A disorder of the endoplasmic reticulum can be either hereditary or acquired (e.g. in CCl 4 poisoning ).
Starvation can cause steatosis, especially in diabetics. Inadequate utilization of glucose causes increased mobilization of fatty acids. A diabetic's body is unable to produce enough lipoproteins, which causes fatty acids to accumulate.

Mitochondrial insufficiency[edit | edit source]
Steatosis occurs when unused MK in the cytoplasm is reesterified to TAG. These then form fat droplets in the cytoplasm, which are bound to mitochondria.
Mitochondrial insufficiency occurs when the carnitine transporter is defective, where the fatty acid cannot enter the mitochondria. A carnitine transporter disorder can be inherited (congenital carnitine deficiency) or acquired ( diphtherotoxin ).
Another cause of reduced utilization of fatty acids is a disorder of beta-oxidation in the mitochondria. The most common reason is ischemia and hypoxia, toxic effects (alcohol), or hereditary diseases. It occurs in energy-demanding cells - skeletal muscle, myocardium, hepatocytes, renal tubule cells.
Steatosis occurs in the liver, for example, during starvation. As already mentioned, there will be an increased mobilization of fatty acids. Mitochondria of hepatocytes are not able to mobilize fatty acids quickly enough and at the same time there is not enough lipoprotein formation. A liver with steatosis has a typical macroscopic appearance and is called a nutmeg liver (resembles a nutmeg on cross section – centroacinosic steatosis).
Hypoxic steatosis of the myocardium is typical for the myocardium (especially with severe anemia). Fat is deposited along the venous sections of the capillary network, causing the typical yellowish heartburn – tiger (or thrush) heart.
A β-oxidation defect (dehydrogenase deficiency) also explains Rey's syndrome, in which sudden deaths of children often occur (e.g. during a respiratory infection, MK is released from adipose tissue and, due to mitochondrial insufficiency, MK and their derivatives accumulate, especially in the liver (massive steatosis - acute liver failure) and the brain (cerebral edema).
Lysosomal dysfunction[edit | edit source]
Increased endocytosis of lipids[edit | edit source]
It depends on the function of histiocytes (lipophages or foam cells) with intensive endocytosis of lipoproteins or other lipid-rich structures ( platelets, erythrocytes, myelin ). Lipids are first deposited intralysosomally (membrane-encased droplets), later in the cytoplasm.
It is mostly cholesterol that is esterified in the cytoplasm and then removed by HDL. Secondary lipopigment ceroid may proliferate. Foamy cells are found in malatic areas of the brain, in the gallbladder mucosa (cholesterolosis - strawberry gallbladder ), in chronic abscesses, atherosclerotic plaques, xanthomas or in the gastric mucosa.
Lipidoses[edit | edit source]
Lipidoses are steatoses due to congenital disorders of lipid metabolism enzymes. These are primarily lysosomal hydrolases, which break down complex lipids (accumulation of lipids in the lysosomal apparatus). As a result, the lysosomal apparatus hypertrophies and acquires a typical honeycomb shape.
- ตับ.jpg
Liver steatosis - macroscopy 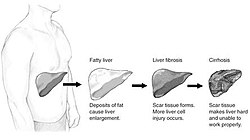
The course of liver damage starting with steatosis 
Steatosis on CT


Hyperlipemia[edit | edit source]
Heterogeneous group of metabolic diseases, when there is an increased level of lipids and lipoproteins in the plasma. We can consider it as extracellular steatosis.
LDL particles are transported in the body to hepatocytes, but also to monocytes, which also have a receptor for chemically damaged LDL. In hypercholesterolemia, the transport of LDL into histiocytes and into the vessel wall increases (smaller molecules pass through the endothelium more easily). Another cause may be an increased synthesis of lipoproteins, a lack of an enzyme that hydrolyzes the transported lipid (on the surface of the endothelium or hepatocytes), or a lack of receptors for LDL on peripheral cells. An increased level of lipoproteins in the blood can accelerate atherosclerosis. Xanthoma with cholesterol crystals Hyperlipemias can be either primary - genetically determined or secondary, when accompanied by other diseases.
Familial hypercholesterolemia (primary HLP)[edit | edit source]
A mutation in the LDL receptor ( cholesterol transport and metabolism ) gene that causes elevated plasma cholesterol levels. Individuals affected by this disease tend to have a threefold (or more) elevated cholesterol level after birth.
The consequence of this disease is premature atherosclerosis of the coronary, cerebral and peripheral arteries, which can lead to cardiovascular disease. In heterozygotes, major complications occur as early as around the age of 40, which can result in death. In homozygotes, it can lead to the death of an individual already around the age of 20.
Other manifestations can be multiple xanthomas, eruptive xanthomas of the skin or tendons, arcus corneae et myringis (interstitial steatosis of the cornea or eardrum).
Diagnosis of steatosis[edit | edit source]
- Laboratory tests – serum transaminases, ferritin.
- Ultrasound - hyperechoic tissue, difficult diagnosis in obese people.
- Biopsy - extra care must be taken (tissues with stenosis are fragile - especially the liver).
Links[edit | edit source]
Související články[edit | edit source]
- Focal large droplet steatosis of the liver (preparation)
- Adipose tissue
- Lipoproteins
- Lipoproteins (clinic)
- Congenital lipomatosis of the pancreas
- Lipidosis
- Obesity
- Lipomas
Source[edit | edit source]
- PASTOR, Jan. Langenbeck's medical web page [online]. ©2005. [cit. 28.9.2010]. <https://langenbeck.webs.com/>.
- NĚMEJCOVÁ, Kristýna. Steatóza, základy buněčné a orgánové patologie mitochondriálních a peroxismálních poruch [online]. ©2018. [cit. 8.11.2018]. <https://pau.lf1.cuni.cz/file/6515/steatoza-nemejcova-2018-cz.pdf>.
Source[edit | edit source]
- POVÝŠIL, Ctibor – ŠTEINER, Ivo. Obecná patologie. 1. edition. Galén, 2011. 290 pp. ISBN 978-80-7262-773-8.
